
---
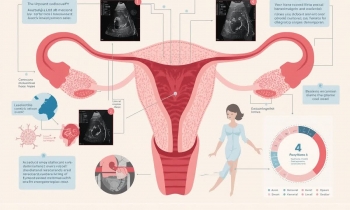
# خونریزی غیرطبیعی رحم (AUB): رویکرد جامع از اپیدمیولوژی و پاتوفیزیولوژی تا تصویربرداری پیشرفته و درمانهای مدرن
همه روزه صبح ها:۸:۳۰ الی ۱۲:۳۰
بعد اظهر ها از ۳ الی ۸:۳۰ به جز پنجشنبه بعداظهر
---
# خونریزی غیرطبیعی رحم (AUB): رویکرد جامع از اپیدمیولوژی و پاتوفیزیولوژی تا تصویربرداری پیشرفته و درمانهای مدرن
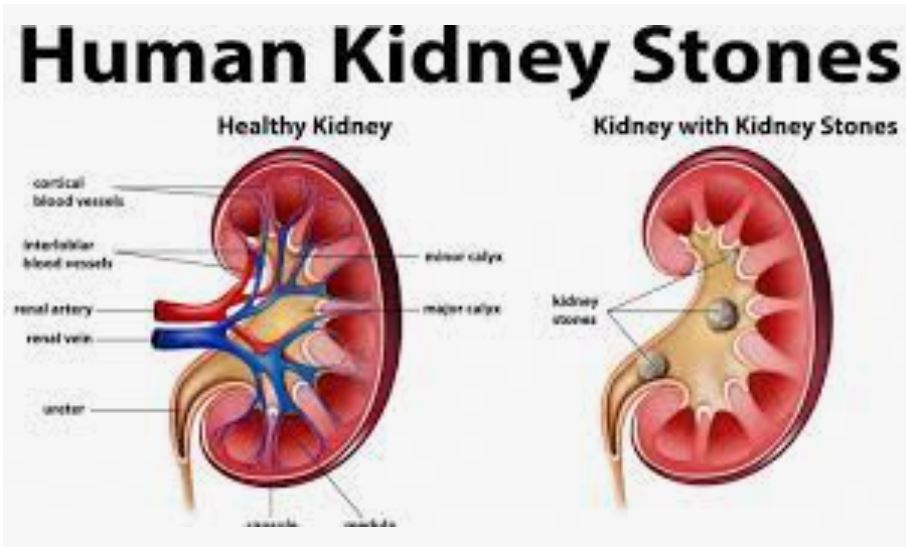
سنگ کلیه NEPHROLITHIASIS
کلمه nephrolithiasis اختصاصاً اشاره به وجود سنگهای کلیوی دارد

------------------------------------------------
مقاله جامع بالینی
بیاختیاری ادرار (Urinary Incontinence)
------------------------------------------------
مقدمه
بیاختیاری ادرار به عنوان نشت غیرارادی ادرار تعریف میشود
تماس با ما :
031-34441004-34427962
اصفهان، ملک شهر، خیابان مطهری،بعد از بانک صادرات و قبل از سه راه نقش جهان،
مجتمع پزشکی سینا - موسسه رادیولوژی وسونوگرافی اسپادانا
ایمیل : info@espadanaradiology.ir